Inheritance from one’s parents refers to the assets they leave to their offspring after they die. It doesn’t matter whether you inherit a fortune or very little material assets, the one thing you will definitely inherit are the particular genetic characteristics or qualities which your family and ancestors had and which you were born with. In biology, inheritance refers to the transmission of genes from parents to their offspring.
While your parent’s wealth may determine your inherited wealth, your parent’s health may also determine your inherited health. Sometimes just a single genetic flaw can have a large effect on your health, such as the way your body deals with fat from your diet. A relatively unknown in the cholesterol family, called lipoprotein(a), can affect hearth health when there are no other obvious risk factors present, such as high blood pressure or high levels of LDL cholesterol. Lipoprotein(a) is not routinely measured when doctors test cholesterol levels by asking for an annual Lipogram.
What are lipoproteins?
Fat is one of the three macronutrients we need from food, the other two being protein and carbohydrates. Fats, called lipids in the biological environment, are insoluble in water and need to be converted to make them water soluble in order to be transported in the watery bloodstream. To make fats water soluble, fat in the diet gets broken down into fatty acids during digestion and these fatty acids get married to protein molecules, the married couple is then called a lipoprotein. Lipoproteins are biochemical assemblies formed from lipid and protein molecules.
Lipoproteins are carrier particles of cholesterol and triglycerides with a specific single apolipoprotein, either ApoB100 or ApoA1, embedded in the wall of the lipoprotein, with different lipoproteins containing different apolipoproteins. Lipoproteins function by permitting the movement of fats through water molecules, such as in the blood stream and other extracellular (outside cells) fluid such as in the lymph, spinal cord, and brain, as well as in fluid inside the cells in the body.
The interior structure of lipoproteins consists of a lipid core, which contains waxy fats called triglycerides and cholesterol that circulate in the blood. Both lipids are crucial to our survival.
- Cholesterol: the liver makes cholesterol, and diet is another source from food, such as animal fats in meat and dairy products. Cholesterol is a major structural component of all cellular membranes (cell walls); is the chemical backbone of many hormones and is also needed to make vitamin D and bile acids.
- Triglycerides: The liver and the intestines in the digestive system make triglycerides from fat and calories. Triglyceride consists of glycerol (sugar alcohol) and fatty acids and are formed through a condensation reaction between one molecule of glycerol and three molecules of fatty acids. Triglycerides are used as an alternative metabolic fuel to glucose in cells and is stored in fat cells to be used as fuel for energy when needed.
The exterior structure of lipoproteins consists of a phospholipid and free cholesterol outer shell with an apolipoprotein, a special kind of protein, embedded in the outer shell.
Types of lipoproteins:
There are four main types of lipoproteins.
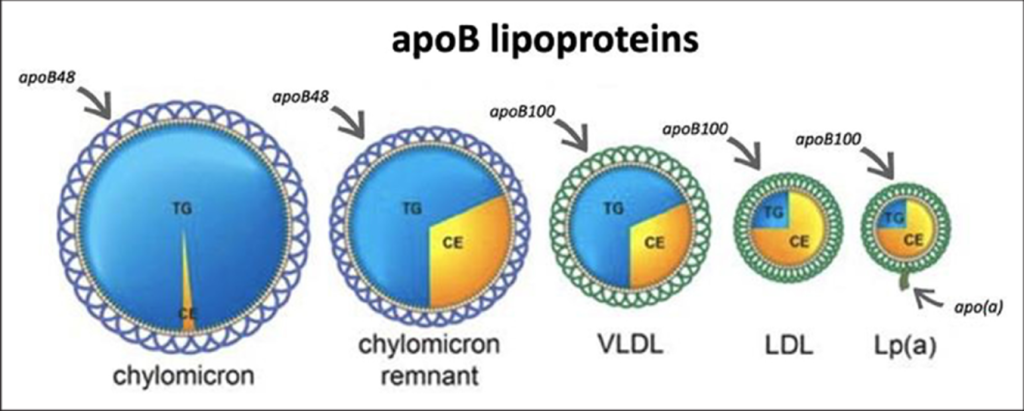
- Chylomicrons: These are large triglyceride-rich lipoproteins produced from dietary lipids (fat), namely fatty acids and cholesterol. They are the largest and most buoyant class of lipoproteins.
- Very low-density lipoproteins (VLDL): This is another type of lipoprotein that carries triglycerides and to a lesser degree cholesterol to the tissues in the body.
- Low-density lipoproteins (LDL): LDLs transport cholesterol after being synthesized in the liver to the cells in the body, where the cholesterol is extracted from the blood by receptors on cell surfaces, which bind with the LDL particles with its attached cholesterol, drawing cholesterol from the blood into the cell, where it is used for various purposes. About 70% of all cholesterol in the blood is carried by LDL particles. There are limits to how much cholesterol a cell can take in and excess cholesterol remains in the bloodstream. LDLs are known as “bad” cholesterol as they are primarily responsible for the atherosclerotic buildup of fatty deposits (also known as plaque) on the walls of blood vessels. (Atherosclerotic refers to plaque buildup that can make blood vessels too narrow for blood to flow freely.)
- High-density lipoproteins (HDL): HDLs probably carry unused or excess cholesterol from the body’s tissues back to the liver, for the cholesterol to be broken down into bile acids and then excreted. HDL is the “good” cholesterol and high levels of HDL can reduce the risk of heart disease.
The type of apolipoprotein present (ApoA1 or ApoB100) in the lipoprotein determines its structure and function:
- ApoA1 is the major apolipoprotein component of HDL (high-density lipoprotein particle) and high levels in the bloodstream usually indicate protective levels and lower risk in terms of atherosclerotic vascular disease.
- ApoB100 is the major apolipoprotein component of low-density lipoprotein (LDL), very-low density lipoprotein (VLDL), and lipoprotein(a). These lipoproteins are associated with a high risk for causing atherosclerotic vascular disease.
How lipoproteins affect atherosclerotic vascular disease:
Aslipoproteins circulate in the bloodstream, triglycerides are rapidly removed by an enzyme (called lipoprotein lipase) in the vascular lining of arteries. The triglycerides that are removed from the bloodstream are used as metabolic fuel in cells and stored in fat tissue in the body, to act as reserves for future energy needs.
The lipoproteins undergo change (remodelling) as triglycerides are progressively removed and thus they become smaller, as the diagram below illustrates. The lipoproteins become even more dense in the form of LDL when most of the triglycerides have been removed, which results in lipoproteins very rich in cholesterol and depleted of triglycerides, while containing one ApoB molecule per carrier particle. ApoB containing lipoproteins, including lipoprotein(a), can easily become trapped in arterial walls to form arterial plaque over time and are directly linked to atherosclerotic vascular disease.
It is advisable to have these important markers for atherosclerotic vascular disease, namely ApoB, and lipoprotein (a), be included in your annual blood tests.
What is Lipoprotein(a)?
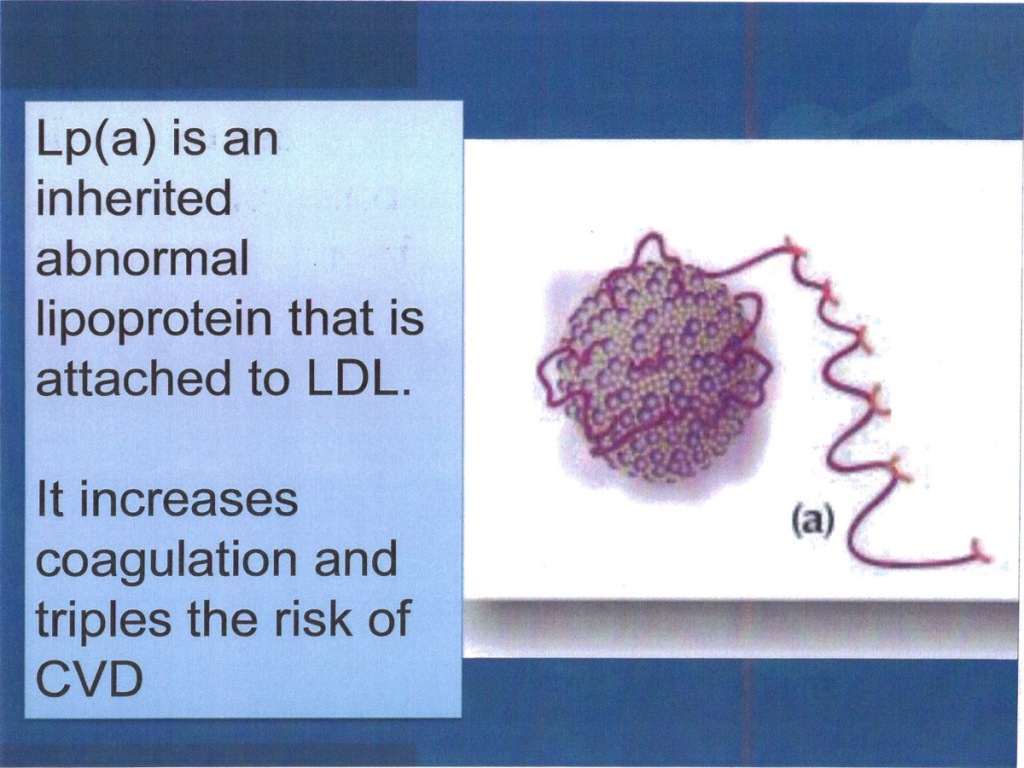
Lipoprotein(a) is a type of LDL cholesterol with a second apolipoprotein that loops around it in segments, which makes the LDL particles more “sticky”, resulting in easier build up in blood vessels, which increases the risk for cardiovascular problems.
Diet and lifestyle can affect LDL and HDL, but your genetic inheritance can include gene changes (mutations) that would make you prone to have high lipoprotein(a) levels, increasing the risk of heart disease at a younger age. As lipoprotein(a) is genetic, it can be detected within the first year of life. It rises throughout childhood and reaches a stable plateau in adulthood. Studies demonstrated about 90% heritability.
It can be measured with a simple blood test and genetic screening is not needed. Results from blood test are reported in mg/dL or nanomoles per liter (nmol/L). Readings above 50 mg/dL or 75 nmol/L are high and increases the risk for conditions such as atherosclerosis, heart attacks, and strokes.
Harvard Medical School says lipoprotein(a) accelerates the buildup of fatty plaque inside arteries as well as inflammation, even more than LDL does, and a high level may double or even triple a person’s risk of a heart attack. It also raises the risk of stroke, and narrowing of the aortic valve, which controls the flow of blood from the heart to the rest of the body.
Are the health risks associated with lipoprotein(a) backed up by science?
While various studies have indicated the cardiovascular risks associated with lipoprotein(a), the results of a very comprehensive study conducted from 2000 to 2019 with a total of 6238 patients, published in May 2024, highlighted the critical importance of lipoprotein(a) The study investigated the association between lipoprotein(a) and heart attack (a blockage of blood flow to the heart muscle), as well as how this association was related to common cardiovascular risk factors for heart disease, known as Standard Modifiable Risk Factors (SMuRFs). The four Standard Modifiable Risk Factors used in this study were hypertension, dyslipidemia (abnormal levels of lipids in the bloodstream), diabetes, and smoking.
In a nutshell, the study found that high levels of lipoprotein(a) were associated with a greater risk for heart disease for patients, even for those without any of the Standard Modifiable Risk Factors. The risk increased if patients with high lipoprotein(a) also had one or more of the Standard Modifiable Risk Factors.
Participants in the study with high lipoprotein(a) had a risk for cardiovascular disease three times higher than those with low lipoprotein(a). Among patients without prior atherosclerotic cardiovascular disease, elevated lipoprotein(a) was linked to a significantly higher risk of heart attack, independent of the presence or the number of Standard Modifiable Risk Factors. The incremental risk posed by high lipoprotein(a) was found to be similar to having two additional Standard Modifiable Risk Factors.
Conclusion
Genetic inheritance is often an unknown factor and doctors may not routinely test for lipoprotein(a) when requesting annual blood lipograms. It may be a good idea to insist that your lipoprotein(a) count be included in your next cholesterol blood tests. In Europe and Canada, guidelines recommend that everyone should get tested for lipoprotein(a) at least once in their lives.
Should the results indicate a high level of lipoprotein(a), be very concerned, as there are currently no simple means of addressing it therapeutically. Elevated lipoprotein(a) is a major risk factor for heart disease, regardless of the presence or absence of other risk factors. All Standard Modifiable Risk Factors are significantly associated with increased risk, with an increased risk with a higher number of these factors. The risk associated with elevated levels of lipoprotein(a) was found to be similar to the risk of having two Standard Modifiable Risk Factors.
As no currently method is able to reduce lipoprotein(a) itself, overall coronary cardiovascular risk can be reduced by treating other modifiable risk factors. Modification of lifestyle factors, such as diet, exercise, smoking cessation, and managing other risk factors such as diabetes and hypertension, can help to reduce overall cardiovascular risk for patients with high lipoprotein(a) concentrations.
According to Dr Mills (Non-invasive and Preventative Cardiologist in Cape Town), new dedicated lipoprotein(a) medications are in phase 3 clinical trials, with promising results. However, none are available yet.
Knowing your lipoprotein(a) status offers a simple estimation of your inherited cardiovascular risk and can help to guide preventative strategies, if needed.
References:
Lipids and lipoproteins in atherosclerotic vascular disease – 2024. Information provided by Dr Philip Mills, Non-invasive and Preventative Cardiologist. Cape Town.
High Lp(a) warrants intervention, even without other cardiovascular risk factors. Published 1 June 2024. Blog by Dr Peter Attia. (www.peterattia.com)
Association of lipoprotein(a) and Standard Modifiable Cardiovascular Risk Factors with incident myocardial infarction. Published 18 May 2024. JAHA. Journal of the American Heart Association. (www.ahajournals.org)
Understanding elevated lipoprotein(a): A focus on cardiovascular risk and screening recommendations. Published 8 March 2024. AJMC. American Journal of Managed Care. (www.ajmc.com)
The latest on lipoprotein(a), an inherited cause of early heart disease. Published 1 February 2023. Harvard Health Publishing. Harvard Medical School. (www.health.harvard.edu)
Lipoprotein. Chemical compound. Published online. Britannica. Encyclopedia. (www.britannica.com)
Lipoproteins. Published online and reviewed 22 May 2022. Cleveland Clinic. USA. (A nonprofit multi-specialty medical centre that integrates clinical and hospital care with research and education.) (www.clevelandclinic.org)
Introduction to lipids and proteins. Published online and last updated 14 January 2024. Endotext. National Centre for Biotechnology Information. US National Library for Medicine. National Institutes of Health. USA. (www.ncbi.nlm.nih.gov)
Cholesterol and lipoproteins 101. Published online. GB HealthWatch. (www.gbhealthwatch.com)
HEALTH INSIGHT