To many a layperson the word “dementia” may conjure up the image of a person who is seen as stark raving mad and locked up in a mental institution. Dementia, however, is not to be confused with mental illness, as it refers to the more serious conditions associated with cognitive decline. Cognitive decline can range in severity from the normal advent of becoming more forgetful as we age, to full blown Alzheimer’s disease and other forms of dementia.
What is cognitive decline?
Cognitive decline is one of the normal processes of aging, just as joints become stiffer and arteries harden. It simply means that the brain doesn’t work as well as it used to, due to the aging of neurons in the brain and the decreased speed at which the brain functions. Cognitive decline manifests itself in three distinctive degrees of severity, starting with the normal cognitive decline due to aging, to mild cognitive impairment (MCI), and the more serious impairment associated with dementia.
Dementia is presented as a loss of cognitive abilities in multiple domains. It results in impairment in the normal activities of daily living and in the loss of independence. Alzheimer’s disease is the most common cause of dementia and is responsible for 60- 80% of dementia cases.
Age-related cognitive decline:
All aging people will experience some degree of cognitive decline and the usual symptoms are forgetfulness, a decreased ability to maintain focus, and a decreased problem solving ability.
While the brain undergo changes as the body ages, mental aging is commonly associated with generally harmless memory problems and forgetfulness. Other changes may include decreases in language skills (can’t find the right word or somebody’s name), also in reaction time, and in the ability to perceive and understand the spatial relationship between real and imagined objects (visual-spatial ability). For the majority of older people this decline is considered a normal part of the aging process. For example, it is quite normal to forget where you have put the car keys, but when you forget what the car keys are used for, you are in trouble!
In order to prevent undue concern when experiencing symptoms of cognitive decline, it is important to be aware of the common symptoms of age-related cognitive decline, which should not be mistaken with the onset of cognitive impairment. Individuals may experience some but not necessarily all of these symptoms. (Source of the following information: Emory University.)
• Intelligence: Abilities such as knowledge or experience that were accumulated over time (referred to as “crystalized” intelligence) tend to remain stable as we age, while abilities that are not based on experience or education (referred to as “fluid” intelligence) tend to decline. (For example: Driving your car still comes naturally, while the latest cellphone functionality evades you!)
• Memory: The memory of events that were stored in the brain over many years tend to remain well preserved and can easily be recalled, while recent memory or the forming of new memories tend to decline with aging.
• Attention: When attention is focused in one area, or simple in nature, it tends to be well preserved. It becomes more difficult as we age when divided attention is required. (Example: Multitasking becomes more difficult. Focusing on a television programme and talking on a phone at the same time becomes more difficult to do.)
• Language: Our vocabulary and verbal abilities are well preserved as we age, but the retrieval process becomes more difficult. It would take longer to find some of the words one wants to use during a conversation, or when trying to recall the names of people or objects. The information is still there, but it is more difficult to retrieve.
• Reasoning and problem solving: Older people tend to maintain their traditional ways of approaching problems and finding solutions. It may take longer to figure out problems that you have not encountered before.
• Speed of processing: The speed at which cognitive (thinking) processes and motor processes (activating and coordinating muscles and limbs) are performed tend to decline with age. The activities involved with these processes can still be performed, but it may take longer to do so.
Mild cognitive impairment:
Mild cognitive impairment (MCI) indicates a condition somewhere between the cognitive decline that is associated with normal aging, and the more serious impairment of dementia and Alzheimer’s disease. This condition causes a noticeable decline in cognitive abilities, such as memory and thinking skills, but the changes are not severe enough to significantly interfere with daily life or the ability to function independently. The decline in cognitive abilities becomes noticeable to both the individual concerned and to family and friends. Although people with MCI have an increased risk of developing dementia, MCI can remain stable and does not necessarily deteriorate into dementia.
Based on the nature of the thinking skills that are affected, the symptoms of mild cognitive impairment can be classified in two broad categories:
• Amnestic MCI primarily affects memory and those affected can experience more memory problems than what is normal for people their age.
• Non-amnestic MCI affects other thinking skills, such as attention, concentration, decision making, judgement, creativity, language skills, visual perception, and navigation skills.
The Mayo Clinic lists the following signs of mild cognitive impairment and the individual may experience any one or more of the following conditions:
• Forgetting things more often.
• Forgetting important events, appointments or social engagements.
• Losing your train of thought or an inability to follow the thread of conversations, books or movies.
• Making decisions or planning a number of steps to undertake a task, even understanding instructions, can become increasingly overwhelming.
• Having trouble finding your way around familiar environments.
• Becoming more impulsive.
• Showing increasingly signs of poor judgement.
• Family and friends start to notice these changes.
• Affected individuals may also experience apathy, depression, anxiety, irritability and aggression.
Dementia.
When cognitive impairment increases in severity to such an extent that it interferes with social interaction, functioning in a working environment, and the ability to live independently, the condition is called dementia. Dementia is a syndrome that is caused by disorders that affect the brain, of which about 90% are caused by Alzheimer’s disease and vascular dementia, or even a combination of the two. Once a person has dementia, it almost always gets worse.
Severe memory decline is usually the first manifestation of dementia, followed by the general loss of cognitive and other brain functions, then comes the need for constant care, and eventually death occurs.
Vascular dementia:
Blockages caused by the buildup of cholesterol plaque (fatty deposits in the arteries) in the brain’s blood vessels can result in memory problems, or even cut off the delivery of oxygen to brain cells – which kills the affected brain cells. Early onset of vascular dementia may not have noticeable initial symptoms with minor brain damage occurring. Blockages in the small blood vessels in the brain can also result in minor strokes that are usually ignored or viewed as “a senior moment.” Vascular dementia causes about 25% of dementia cases.
Alzheimer’s disease:
Alzheimer’s disease usually starts with slowly losing some of the advanced mental functions, such as the ability to do mathematical activities related to household finances and word recall. Mood changes and behavior changes are also witnessed early in the disease. As the disease progresses, disorientation and serious memory loss occurs. In the later stages of Alzheimer’s the patients often do not speak or move anymore.
While vascular dementia results from plaque in the blood vessels, Alzheimer’s disease results from loss of the brain’s neurons and synapses. The brain of an Alzheimer’s patient displays tangles and plaques that affects the transfer of impulses between neurons. The tangles and plaques are the main contributors to Alzheimer’s disease and these were identified by researchers as tau protein tangles and amyloid-beta plaque buildup. When these tangles and plaques starts to form in the brain, it may not immediately affect memory, but these individuals are at a higher risk of developing Alzheimer’s disease.
According to Harvard Medical School, tau is a normal protein that transports nutrients into brain cells and move waste products out of brain cells. Aging or errant genes can cause tau to become abnormal, resulting in pieces of the tau protein to tangle and clump together. In this event the nutrients and toxic waste products can no longer move freely within brain cells and these cells may eventually die. The neurofibrillary tangles are bundles of filaments composed primarily of tau protein, which often first form in the regions in the brain that is used for memory, but can soon spread across the rest of the brain.
The fatty membrane that surrounds brain cells contain a protein molecule called beta-amyloid, which can cause plaque buildup outside the cells of the brain when it clumps together. Dr. Dale Bredesen describes the plaque buildup as “sticky globs of amyloid” that can gung up the spaces (the synapses) between brain neurons. As neurons communicate with each other via the synapses, the damage caused by the plaque to the synapses can result in synapses that stops functioning, which have devastating consequences for the transfer of signals (communication) between neurons. This can ultimately kill neurons.

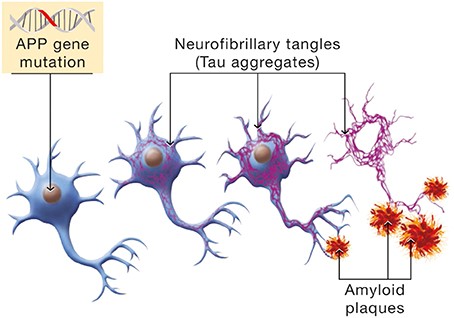
These two protein aggregates that can interfere with the normal neurological functioning of the brain are not the only factors at play. A genetic predisposition can also contribute to the risk of developing Alzheimer’s disease. A gene that is identified as APOE has a mutation (variant) called the E4 that is the strongest known genetic risk factor for Alzheimer’s. People who carry one ApoE4 (inherited from one of your parents) have a 30% increase in lifetime risk for Alzheimer’s, while those who carry two copies of ApoE4 (inherited from both parents) have a risk factor of more than 50%. In comparison, people who carry no copies of ApoE4 only have a 9% risk of developing Alzheimer’s.
In addition, the brain can become insulin resistant. At present vital and an immense amount of research is trying to determine the role of brain insulin resistance in the neurodegeneration that occurs in Alzheimer’s. Is it a consequence or a cause or part of the tau tangles and amyloid-beta plaque pathology?
Insulin resistance, whether in the brain or elsewhere in the body, is defined as the failure of cells to respond to insulin. This could be due to an impaired molecular signaling response or a decreased number of insulin receptors that occurs with aging.
Despite glucose being the major source of energy for the brain, the uptake and use of glucose by neurons is only influenced by insulin, but it is not dependent on it.
The widespread distribution of insulin receptors in the human brain, especially in the hypothalamus, hippocampus, cerebral cortex, thalamus and cerebellum, suggests that insulin signaling has important and diverse roles in the brain. Studies have shown that in the hypothalamus, for example, insulin plays a role in helping to regulate eating behaviour and energy expenditure.
Insulin receptors are found on both neurons and glial cells in certain regions of the brain. The latest research has shown that insulin plays a role in synaptic transmission, neuronal and glial metabolism, neuro-inflammatory responses, and that insulin also promotes neuronal survival by inhibiting apoptosis (programmed cell death).
Accumulating evidence from animal models is emphasizing more and more the significant role that insulin deficiency and insulin resistance of the brain plays as mediators of the neurodegeneration seen in Alzheimer’s disease.
Insulin resistance of the brain is commonly referred to as Type 3 diabetes.
Conclusion:
The good news is that not everybody shows a progression of cognitive decline as they age. Most people will only experience the generally harmless “forgetfulness” and other memory problems that are experienced from age 60 onwards. Studies show that less than 20% of people over age 65 may develop mild cognitive impairment, while around 10% of people age 65 and older develop Alzheimer’s disease.
Sources:
Age related cognitive decline. Published online. LifeExtension. (www.lifeextension.com)
Mild cognitive impairment (MCI). Published online 23 August 2018. Mayo Clinic. (www.mayoclinic.org)
Get the facts about memory loss. Published online August 2019. Harvard Men’s Health Watch. Harvard Medical School. (www.health.harvard.edu)
Mild cognitive impairment (MCI). Published online. Alzheimer’s Association (USA). (www.alz.org)
What is mild cognitive impairment? Published online. National Institute on Aging. National Institute of Health. US Department of Health & Human Services. (www.nia.nih.gov)
What to do about mild cognitive impairment. Published online December 2017. Harvard Men’s Health Watch. Harvard Medical School. (www.health.harvard.edu)
Cognitive skills & normal aging. Published online. Goizuetta Alzheimer’s Disease Research Center, Emory University. Atlanta, USA. (www.alzheimers.emory.edu)
The end of Alzheimer’s. Dr Dale Bredesen. Book published 2017. Penguin Random House UK. 307p.
Insulin resistance in the brain. Published online and updated 9 April 2019. APOE4. (www.apoe4.info/wiki)
HEALTH INSIGHT