“The most sophisticated, complex system in the universe – the human brain!”
There is currently no medicine (drug) available to prevent, slow down, or cure the cognitive decline that is associated with dementia, of which Alzheimer’s disease the most common form.
A family member once observed, while interacting with her mother, a full-blown Alzheimer’s disease patient: “I have lost my mom while she is still alive.” But what if her mother could have been helped with the onset of Alzheimer’s, to not only prevent her from forever getting lost in the dense fog overwhelming her brain, but to stop the decline and even reverse the condition?
More than three decades of research by a group of neuroscientists in the USA, guided by neuroscientist Dr Dale Bredesen, into the basic mechanisms of neuro-degeneration and the accompanying chemical processes that take place in the brain when Alzheimer’s and other forms of cognitive decline occur, has determined that Alzheimer’s is not a single disease as the symptoms may indicate, but results from a wide range of different biochemical processes. This insight into the magnitude of biochemical processes that affect cognitive decline and dementia, has also resulted in understanding how to address these biochemical processes in order to halt, prevent and even reverse the cognitive impairment associated with Alzheimer’s during the mild to moderate stages of the disease. Sadly, there is no remedy once too much neurological damage has occurred.
Neurotransmitters in the normal brain:
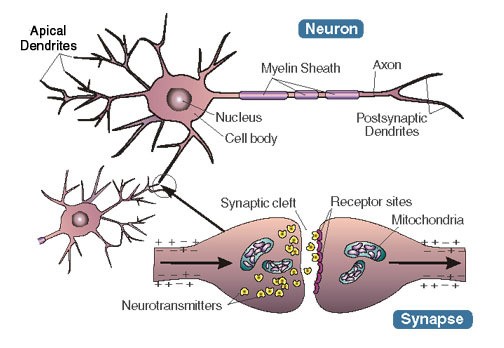
The brain consists more than 100 billion nerve cells (neurons), which are linked and communicate with other neurons through trillions of connections. Sensory input to the brain is sent via nerve impulses between neurons, to different parts of the brain. These complex electrochemical signals, or nerve impulses, form the basis of the brain’s essential functions, such as forming memories and thoughts, producing and/or initiating actions, as well as assisting to interpret the world around us. Neurons are the basic building blocks of the body’s nervous system.
Neurons communicate with each other via these electrochemical signals. The electrical events that take place across the synapses between neurons are called action potentials. The chemical part of this communication process starts when an action potential reaches the synaptic cleft (“gap”) between neurons, and causes neurotransmitters (”chemical substances”) to be released from the neuron’s axon into the cleft. After crossing the cleft, the neurotransmitters attach to receptors on the dendrites of the receiving neuron. The synapse can be seen as the junction between the axon of one neuron and the receiving dendrite of another neuron; where the electrochemical communication processes take place and signals are transmitted.
Neurotransmitters in the Alzheimer’s brain:
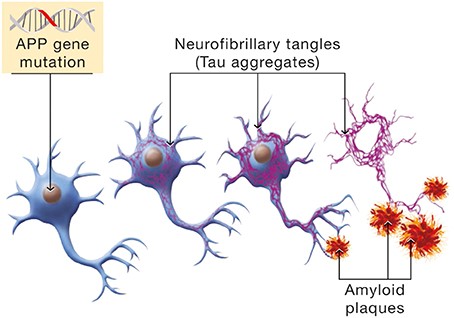
Alzheimer’s disease results from loss of the brain’s neurons and synapses. The brain of an Alzheimer’s patient displays tangles and plaques that affects the transfer of impulses between neurons. The tangles and plaques are the main contributors to Alzheimer’s disease and these were identified by researchers as tau protein tangles and amyloid-beta plaque build-up. When these tangles and plaques start to form in the brain, it may not immediately affect memory, but these individuals are at a higher risk of developing Alzheimer’s disease.
Tau is a normal protein that transports nutrients into brain cells and move waste products out of brain cells. Aging, or errant genes, can cause tau to become abnormal, resulting in pieces of the tau protein to tangle and clump together. In this event the nutrients and toxic waste products can no longer move freely within brain cells and these cells may eventually die. The neurofibrillary tangles are bundles of filaments composed primarily of tau protein, which often first form in the regions of the brain that is used for memory, but can soon spread across the rest of the brain. The fatty membrane that surrounds brain cells contain a protein molecule called beta-amyloid, which can cause plaque build-up outside the cells of the brain when it clumps together. Dr Dale Bredesen describes the plaque build-up as “sticky globs of amyloid” that can gung up the spaces (the synapses) between brain neurons. As neurons communicate with each other via the synapses, the damage caused by the plaque to the synapses can result in synapses that stops functioning, which has devastating consequences for the transfer of signals (communication) between neurons. This can ultimately kill neurons.
These two protein aggregates, that can interfere with the normal neurological functioning of the brain, are not the only factors at play. A genetic predisposition can also contribute to the risk of developing Alzheimer’s disease. A gene that is identified as APOE has a mutation (variant) called the E4 that is the strongest known genetic risk factor for Alzheimer’s. People who carry one copy of ApoE4 (inherited from one of your parents) have a 30% increase in lifetime risk for Alzheimer’s, while those who carry two copies of ApoE4 (inherited from both parents) have a risk factor of more than 50%. In comparison, people who carry no copies of ApoE4 only have a 9% risk of developing Alzheimer’s.
The real causes of Alzheimer’s:
While the neuron-strangling tau tangles and the build-up of amyloid plaques are manifestations of Alzheimer’s in the brain, the Bredesen research has found a multitude of biochemistry related conditions that are at the root of the disease. The brain has the natural ability to fight outside threats, but when these threats are chronic and multiple in nature, continuing unrelenting and intense, the brain’s natural protective mechanisms responds accordingly and can cause the harm that is associated with Alzheimer’s.
According to the Bredesen findings, Alzheimer’s is what happens when the brain tries to protect itself from of a wide range of metabolic and toxic threats, that can be summarized in three main categories:
• Inflammation (resulting from dietary sources, infection, or many other causes).
• A decline in, or shortage of nutrients, hormones and other brain-supporting molecules.
• Exposure to toxic substances such as metals (for example, mercury) or biotoxins (which are poisons produced by microbes, such as moulds).
The brain is usually able to protect itself from these threats. When these threats are chronic and intense in nature, the intrinsic defense mechanism in the brain that fights invading pathogens by producing amyloid, crosses the line from defense mechanism into causing harm to the brain’s synapses. When high concentrations of amyloid-beta accumulate in the brain, it triggers the defense receptors to reduce the connections (synapses) and ultimately kill the neurons.
The crucial role that amyloid-beta plays in the brain:
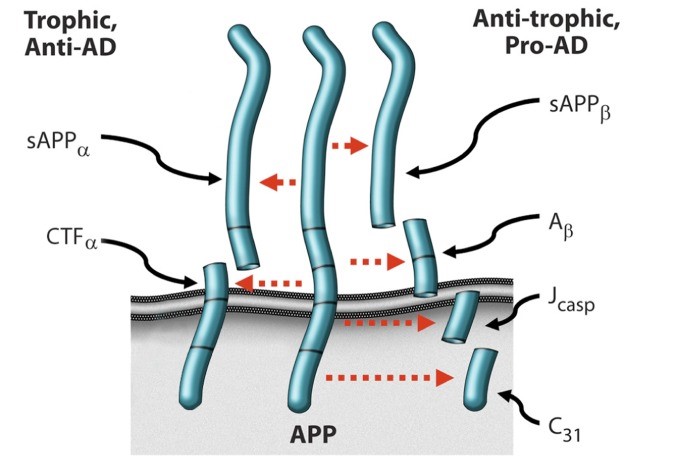
• Amyloid precursor protein (APP) is a neuron receptor molecule produced by the neurons.
• Once produced by the neurons, APP is “cut” by molecular scissors called proteases and the way it is cut determines whether it will harm or protect the synapses. The proteases process will either cut in a single site along APP’s 695 amino acids, or cut in three sites.
• Cutting at a single site has a synapse-supporting function by producing two peptides that maintain synaptic connections and nourish the neuron’s axons and dendrites, as well as blocking the neuron’s built-in “suicide program” of downsizing synapses and neurons when under threat.
• However, cutting the APP’s 695 amino acids at three sites, produce four different peptides that starts the synapse-destroying processes that lie at the bottom of Alzheimer’s disease, such as the loss of synapses; the shriveling up of the parts of the neurons that extends to connect to other neurons; as well as activating the neuron’s suicide programme.
• The specific molecules that bind to APP determines whether it is cut in a single site or at three sites. When APP grabs a molecule called netrin-1, it gets cut at a single site. When APP grabs amyloid-beta, it gets cut at three sites and produces four Alzheimer’s causing molecules, one of which is amyloid-beta which then binds to APP and activates APP to produce more amyloid-beta. This becomes a vicious circle with devastating effects on the synapses and neurons.
• APP responds to dozens of molecules and they are all linked to the potential to develop Alzheimer’s, for example oestrogen, testosterone, thyroid hormone, insulin, inflammatory molecule, vitamin D, and many others. They all exert leverage at the crux of the Alzheimer’s pathway.
• APP is a master dependence receptor that integrates the inputs of many receptors (and is not just a single input receptor, such as for example the vitamin D or testosterone receptors). When APP learns from the various dependence receptors that they are not getting sufficient input, it sends out the signal for the destructive molecules to start downsizing the synapses, as part of the brain’s defense mechanism.
Potential contributors to Alzheimer’s:
A small minority of cases of cognitive decline may have a cause other than neurodegenerative processes, such as a brain tumor. This possibility can be excluded with MRI or CAT scans.
The Bredesen research projects have identified at least 36 molecular mechanisms that affects the way either synapse-supporting or synapse-destroying molecules are formed in the brain. When synapse destruction overwhelms synapse maintenance and formation, the brain goes into protective mode and starts to downsize (by destroying synapses and neurons) in order to preserve only the functions it needs to stay alive, such as breathing and maintaining body temperature, to the detriment of other abilities that make us human, such as thinking, remembering, understanding and imagining. At the final stage of the downsizing process, death occurs.
In broad terms, Alzheimer’s results from a protective response to one or more of the three major subtypes of factors that leads to Alzheimer’s: – inflammation; suboptimal nutrients and hormone levels; and toxic compounds. Metabolic evaluation (such as blood tests) can pinpoint which of these major subtypes of Alzheimer’s, or how many of them, are driving any individual patient’s cognitive decline.
1. Inflammation: The body’s immune system mounts an inflammatory response when under acute threat from invading pathogens (such as viruses, bacteria, fungi, parasites). When the threat is chronic, the inflammatory response is continuously activated, leading to the accumulation of amyloid in the brain. Inflammation is also triggered by food such as trans fats (artificial fats in baked pre-packaged foods and fried foods) or sugar. Sugar toxicity (high intake) is accompanied by insulin resistance, which is intimately linked to Alzheimer’s.
2. A shortage of brain-boosting nutrients, hormones and other cognition-supporting molecules: In order to function optimally, the brain needs optimal levels of neuron- and synapse-supporting factors, which includes a wide range of nutrients and hormones.
3. Toxic exposure: When the brain is infiltrated by toxic metals such as copper and mercury, or by biotoxins such as produced by moulds, amyloid plays a protective role by binding to these toxins to prevent them from damaging the neurons. Chronic exposure to toxic substances, however, results in the brain churning out too much amyloid.
Alzheimer’s can be reversed:
Any treatment regime for Alzheimer’s starts with identifying which of the wide variety of molecular mechanisms (according to Dr. Bredesen there are at least 36) amongst these three subtypes are potential threats to a particular patient’s brain. The patient’s brain responds defensively to these potential threats by activating the synapse-destroying molecules. Once these potential threats have been identified, the treatment process would be aimed at removing the specific contributors and fending off any other potential attackers. Once the triggers for amyloid production for a specific patient have been eliminated, a treatment regime can start to rebuild the synapses that have already been destroyed, unless the damage is so severe that it is irreversible.
Our bodies are complex systems where cells and physiological biochemistry work as a whole. By correcting and preventing imbalances in our basic biochemistry, dysfunctions can be prevented and improved before a disease has taken over. In the event of Alzheimer’s, finding the real cause of the cognitive decline allows the opportunity to fix any imbalances before it becomes irreversible. Late in the progression of Alzheimer’s there is such a huge loss of synapses and neurons that correcting the causes won’t be able to reverse the cognitive decline. Identifying and evaluating all of the risk factors and potential contributors for cognitive decline entails the use of brain scans, genetic testing and a wide range of blood tests for a comprehensive metabolic evaluation that will pinpoint which factors are driving the patient’s cognitive decline:
• Homocysteine
• Vitamins B6, B12 and Folate
• Insulin resistance
• Inflammation
• Vitamin D
• Hormonal status (thyroid, testosterone, oestrogens and progesterone)
• Metal detection (copper-zinc ratio, red blood cell magnesium, selenium and glutathione, heavy metals such as mercury, arsenic, lead and cadmium)
• Sleep and sleep apnea
• Cholesterol and other lipids
• Vitamin E
• Vitamin B1 (thiamine)
• Gastrointestinal permeability (“leaky gut syndrome”)
• Blood-brain barrier permeability
• Autoantibodies
• Toxins
• Mitochondrial function
• Body mass index (BMI)
• Other considerations such as historical and lifestyle features.
Dr Bredesen refers to his treatment protocol as the ReCODE (Reverse Cognitive Decline), which addresses each of the biochemical, genetic and other factors that are causing the synaptic destruction in a specific patient. At the time his book The End of Alzheimer’s was published in 2017, his ReCODE protocol has already been successfully used to improve the cognitive decline of more than 200 patients.
The basic concepts that applies to the ReCODE treatment protocol are:
• Go beyond normal levels to optimal levels for each abnormality that was identified.
• Address as many abnormalities as possible.
• Address the root cause.
• The ReCODE programme is personalized for each patient, based on the laboratory values.
• There is a threshold effect – once enough of the network components have been optimized, it reaches the tipping point where synapse destruction can be halted, and reversed to synapse maintenance and preservation.
• The programme is broken up into phases.
• The earlier treatment starts, the greater the chance for reversal.
• People who responds the best to the programme are those who are at risk because of their genetic ApoE status, but who do not yet have symptoms; people with early mild cognitive impairment; people with early Alzheimer’s disease; and people with first signs of cognitive decline who are otherwise healthy.
Apart from the 36 metabolic factors identified by Dr. Bredesen, a number of lifestyle factors can also play a role in cognitive decline.
• People who are physically active, especially doing regular aerobic exercise, have reduced risks for cognitive decline.
• People who smoke are at a higher risk for a number of serious health conditions, including cognitive decline.
• Excessive alcohol consumption is a significant risk factor for cognitive decline.
• Stress increases levels of cortisone, which at chronically high levels are toxic to the brain.
• Lifelong learning and mental stimulation have been associated with cognitive health, and higher levels of cognitive activity in later life have been linked to the delayed onset of cognitive impairment.
• People who are overweight or obese in midlife may have an increased risk of cognitive decline.
• Good-quality sleep of close to eight hours every night is known to improve overall health and may play a role in preventing cognitive decline.
• A healthy nutritious diet plays a crucial role in brain health.
(Please see the relevant Health Insight blogs: The Mediterranean Way; and The Best Diets (2019).
Note: For background information on the brain, please also read the Health Insight blogs Cognitive Decline and Dementia, and Memory.
Sources:
The End of Alzheimer’s. The first programme to prevent and reverse the cognitive decline of dementia. Author: Dr Dale Bredesen. Book published 2017 by Penguin Random Hous
Reversal of cognitive decline: A novel therapeutic programme. Published online 27 September 2014. National Center for Biotechnology Information. US National Library for Medicine. National Institutes of Health. (www.ncbi.nlm.nih.gov)
Staving off dementia when you have mild cognitive impairment. Published in the Harvard Health Letter, April 2018. Harvard Medical School. (www.health.harvard.edu)
Protecting against cognitive decline. Published online. Harvard Medical School. (www.health.harvard.edu)
Seven lifestyle interventions evaluated by the World Health Organization for preventing cognitive decline and Alzheimer’s. Published online 14 August 2019. Alzheimer’s Drug Discovery Foundation. (www.alzdiscovery.org)